[This is a continuation of Condoms & Ethnicity I]
UPDATE: 2013-10-27: A latter portion of the post has been invalidated, my apologies.
UPDATE: 2013-08-31: The claim at this link is incorrect. The WHO report was written by an Australian condom manufacturer who arbitrarily used these three studies to propose that different sizes may be preferred by persons in different countries. These studies do NOT indicate that penile width differs by ethnic group as none of the studies were performed by medical professionals nor were they replicated.
The Family Health International (FHI) & JP Rushton
In a FHI monograph by Spruyt (1996), we read:
The World Health Organization bases its specifications for condom width on consumer preference and penis size, citing three studies. Taken together, the studies show significant variations in penis size within all population groups, but also indicate that men of African descent on average have a slightly wider and longer penis size, Caucasian men have a medium size, and Asian men a slightly narrower and shorter size (WHO).
Based on the consideration that anatomical differences exist among regions, a series of FHI studies were conducted in three Asian countries to compare small and standard width condoms (49 mm and 52 mm), and in three African countries to compare larger and standard width condoms (55 mm and 52 mm). Among the African sites, breakage rates were slightly higher and slippage was slightly lower for the smaller of the two condoms being compared. (Joanis) However, results from the Asian sites were inconsistent. (Neupane; Andrada) Moreover, almost none of the differences in breakage and slippage rates from either the Asian or African sites were statistically significant. Thus, results from these studies pertaining to penis size and condom failure were inconclusive.
So the FHI found it necessary to launch three studies based on one page of a WHO condom report. The report itself (WHO 1998) is most interesting and highlights the need for not accepting data at face value.
ANALYSIS OF THE WHO ETHNIC PENILE DIMENSIONS
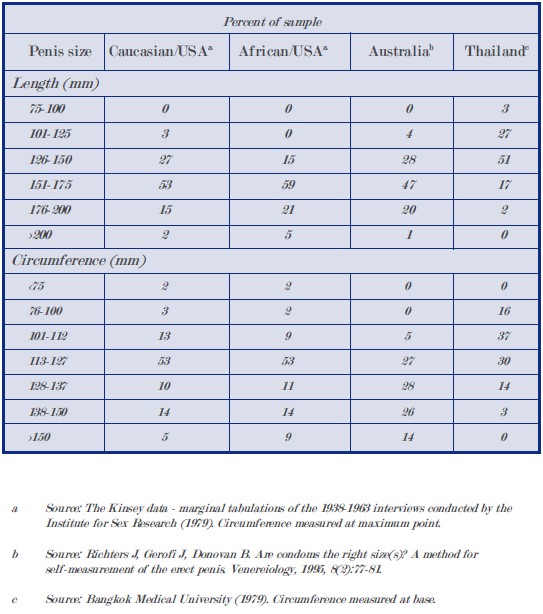
The table below is the one page WHO listing of three studies which purport to show ethnic variations in both penile length and girth.
Unsurprisingly, infamous race realist Rushton (2000) poses questions and answers using the same WHO data in his book Race, Evolution, and Behavior: A Life History Perspective. Two questions are of importance to penis variations and source analysis.
Q: Doesn’t the evidence on race and penis size come from 19th Century stories by racist Europeans in colonial Africa?
A: The earliest findings come from the Arabic explorers in Africa and one study by a French army surgeon originally published in 1898. More up-to-date information comes from the World Health Organization. Their studies show the same three-way race pattern as do all the other studies.
Q: Isn’t the material on race and sex a kind of pornography? Isn’t race controversial enough without bringing sex and AIDS into the picture?
A: One World Health Organization study I mentioned in the previous answer examined penis size in order to provide the right size condoms to slow the spread of AIDS. Finding out which groups are most at risk for sexually transmitted diseases can help slow their spread and save lives.
ANALYSIS: The WHO did not study penis sizes. It relied on three separate studies, two of which were not peer-reviewed and the data was included as “Appendix III” (which should have alerted Rushton that this was not an original study). The first study references Africans in the US (not Africa!) and Europeans in the US (not Europe!), the second Europeans in Australia (not Europe!) and the third, Thais.
The first study is Alfred Kinsey’s flawed self-reported study on incarcerated males (a highly truthful bunch no doubt). The sampling, methodology and measurements are biased.
The reference for Asians is stated as an unpublished study by Bangkok Medical University (Muangman 1978) and nothing is known about the sample size or methodology (besides that prostitutes measured with paper tapes). Thus this is another biased study and does not represent the average Thai male.
The Aussie study was peer-reviewed but submitted a method for self-measurement. For a sample of 156, they found an average erect length of 15.99 cm or 6.3” (Richters, Gerofi & Donovan 1995 as mentioned in Mondaini et al. 2002) which is larger than Rushton’s upper European limit of 6″. While this value of 15.99 cm is the largest value from 8 different studies (Promodu et al. 2007), it does seem accurate given another study.
Estimated applicability of Rushton’s values to the WHO data
Rushton proposes to have found the following: East Asians: 4 to 5.5″ (10.2 to 14.0 cm) in length and 1.25″ (3.2 cm) in diameter, Europeans: 5.5 to 6″ (14 to 5.2 cm) in length and 1.5″ (3.8 cm) in diameter and Africans: 6.25 to 8″ (15.9 to 20.3 cm) in length and 2″ (5.1 cm) in diameter. In other words, the average European is 21% longer and 50% thicker than the average East Asian, while an average African is 50% longer and 60% thicker.
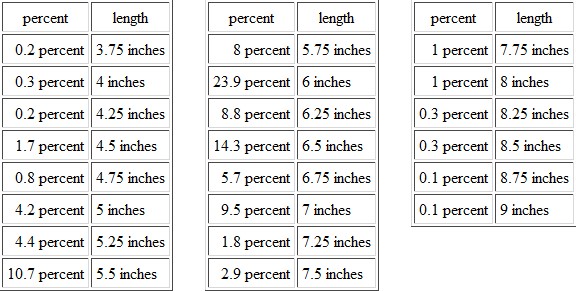 If this link is accurate (see pic above), Rushton’s US European length claim only correlates some 43% with that of Kinsey’s data. The Thai study found 51% with 5 to 5.9” penises which correlates more than that for Europeans and yet is larger than his 4 to 5.5″ assertion.
If this link is accurate (see pic above), Rushton’s US European length claim only correlates some 43% with that of Kinsey’s data. The Thai study found 51% with 5 to 5.9” penises which correlates more than that for Europeans and yet is larger than his 4 to 5.5″ assertion.
The WHO girth data gives 29% of Euro-Americans, 68% of Euro-Australians, 34% of Afro-Americans and 17% of Thais having circumferences above 5”. Why so large a value for Aussie-Europeans compared to US Europeans? A portion of the WHO states:
Condoms are made in various widths. Based on studies in Australia, Thailand and the USA, and the experience of major agencies, the wider condoms (flat width 52-55 mm) will be preferred in Australia, Africa, Europe, Latin America, the Middle East and North America, and the narrower condoms (47-51 mm) will be preferred in several Asian countries (see Appendix III). Other widths are also made for small specialized markets.
[This portion has been invalidated, see comments below] While wondering which Asian countries are being referenced and if any are not, one would be inclined to treat the ‘experience of major [unnamed] agencies’ as authoritative. The Asian preferred circumference range is 147.7 to 160.2 mm. Similarly, the non-Asian preference circumference is 163.4 to 172.8 mm. From the data, 95% of Euro-Americans, 91% of Afro-Americans, 86% of Euro-Australians and 100% of Thais have penile girths less than or equal to 150 mm. Why then would there be a preference among Africans and Europeans for condoms some 13.4 to 32.8 mm larger?
2013-02-22, update: The answer to the last question can be found here, here and here.
SOURCES:
Andrada A, Ravelo N, Spruyt A, et al. 1993. Acceptability and Functionality of Standard and Smaller Latex Condoms during Human Use: Philippines. Durham, USA: Family Health International.
Joanis, C., Brookshire, T., Piedrahita, C., Steiner, M., Diakite, M., and J. Esibi. 1990. Evaluation of Two Condom Designs: A Comparison of Standard and Larger Condoms in Ghana, Kenya, and Mali. Durham, USA: Family Health International.
Mondaini, N., Ponchietti, R., Gontero, P., et al. 2002. Penile length is normal in most men seeking penile lengthening procedures. International Journal of Impotence Research 14: 283-286.
Muangman, D. 1978. Report on measurement of Thai male genital sizes and recommendation for appropriate condom usage [unpublished paper]. Bangkok Faculty of Public Health, Mahidol University.
Neupane, S., Abeywickrema, D., Martinez, K., et al. 1992. Acceptability and Actual Use Breakage and Slippage Rates of Standard and Smaller Latex Condoms: Nepal and Sri Lanka. Durham, USA: Family Health International.
Promodu, K., Shanmughadas, K., Bhat, S., and K. Nair. 2007. Penile length and circumference: an Indian study. International Journal of Impotence Research 19: 558-563.
Richters J., Gerofi J., and B. Donovan. 1995. Are condoms the right size(s): a method for self measurements of erect penis. Venerology 8: 77-81.
Rushton, J.P. 2000. Race, Evolution, and Behavior: A Life History Perspective. Port Huron, USA: Charles Darwin Research Institute.
Spruyt, Alan. 1996. User Behavior and Characteristics related to Condom Failure in McNeill, E., et al. (eds.) The Latex Condom: Recent Advances, Future Directions. Durham, USA: Family Health International. http://www.fhi360.org/en/RH/Pubs/booksReports/latexcondom/behavcharac.htm [accessed: 2012-01-15].
WHO. 1998. The Male Latex Condom: Specification & Guidelines for Condom Procurement. WHO & Joint UN Programme on HIV/AIDS. http://whqlibdoc.who.int/hq/1998/WHO_RHT_FPP_98.15_spec&guidelines.pdf [accessed: 2012-01-23].





